The Illusion of a Miracle Cure
A paralyzed man moves his hand using nothing but his thoughts. The headlines write themselves. When Feinstein Institutes for Medical Research announced they had successfully implemented a double neural bypass on a quadriplegic patient, the mainstream press treated it as an overnight miracle. They painted a picture of a solved problem, a straight line from laboratory to living room.
It is a lie of omission.
The achievement is a monumental feat of biomedical engineering, but treating it as an immediate cure misleads millions of families living with spinal cord injuries. The reality behind the double neural bypass is a messy, expensive, and grueling compromise between human biology and silicon. It is not a cure for paralysis. It is a highly tethered, temporary bridge built over a permanent chasm. Understanding what actually happened in that operating room requires stripping away the public relations gloss and looking at the raw infrastructure keeping this technology alive.
Anatomy of the Double Bypass
To understand why this system is both a triumph and a prisoner of its own design, you have to look at how it circumvents a broken spinal cord. In a healthy body, the brain sends electrical signals down the spinal cord to the limbs, and the limbs send sensory feedback back up. Injury smashes this highway.
The double neural bypass does not repair the highway. It builds an alternate flight path.
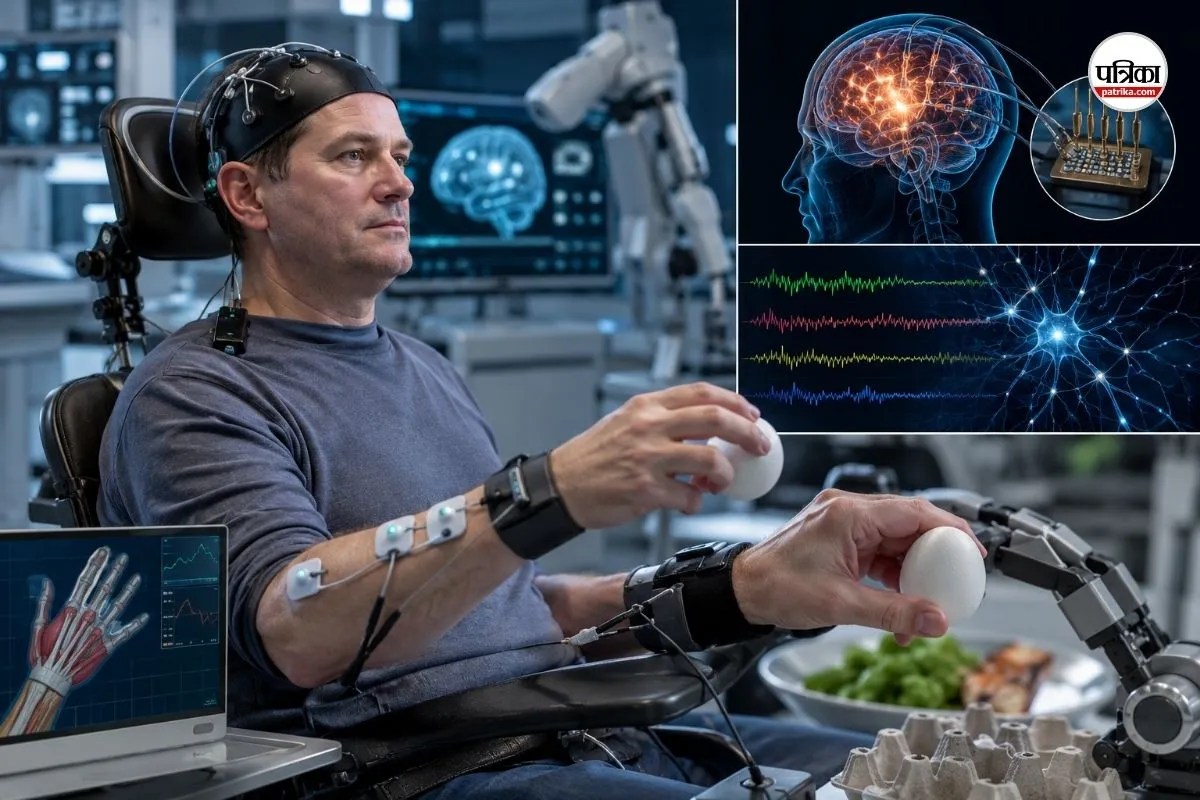
[Brain: Motor Intent] ---> [Implants] ---> [AI Computer] ---> [Electrode Patches on Forearm]
|
v
[Brain: Sensory Input] <-- [Implants] <-- [Fingertip Sensors] <-- (Physical Movement)
Surgeons implanted five microchips directly into the patient's brain—specifically in the areas responsible for hand movement and fingertip sensation. When the patient thinks about moving his hand, the brain chips detect the electrical firing of his neurons.
Those signals travel out of his skull through physical ports. They plug into an external computer running machine learning algorithms. The computer decodes the intent, translates it into electrical commands, and routes those commands to electrode patches placed on the patient's forearm. The forearm muscles contract. The hand closes.
That is only the first bypass. The second bypass goes backward. Sensors on the patient's fingertips detect the pressure of an object and send that data back to the computer, which translates it into signals delivered to the sensory chips in his brain. The patient "feels" what he is touching.
It works. It is real. But it is entirely dependent on a massive stack of external hardware that no patient can take home.
The Power and Processing Bottleneck
The algorithms decoding these neural patterns require immense computational power. We are talking about translating millions of firing neurons in real time. Right now, this happens on a server stack. The patient cannot walk down the street with this system because the system requires a room full of engineering equipment and a team of technicians to keep the calibration from drifting.
The Biological Clock
The human body hates foreign objects. The moment those microchips are implanted into the brain, the immune system begins its slow, inevitable defense. Glial cells surround the electrodes, forming scar tissue. Over time, this tissue insulates the chips, dulling the electrical signals. History shows us that these types of invasive brain-computer interfaces have a shelf life. Signals degrade. Eventually, the implants blind themselves.
The Economics of Exclusion
Who actually gets this technology? Right now, the answer is virtually no one.
Medical breakthroughs of this scale are staggeringly expensive. The cost of the surgeries, the custom-fabricated microchips, the proprietary software, and the hundreds of hours of post-operative engineering support run into millions of dollars per patient. This is clinical research, funded by grants and venture philanthropy. It is not a product.
If this technology ever reaches the commercial market, it faces an systemic healthcare barrier. Insurance companies do not traditionally fund experimental, high-maintenance neural prosthetics that require constant calibration. We risk creating a dystopian divide where a microscopic fraction of wealthy patients can buy back a percentage of their mobility, while the rest of the paralyzed population is left with standard physical therapy and wheelchairs.
Furthermore, the focus on high-tech neural bypassing sucks the oxygen out of the room for simpler, more scalable solutions. Epidural stimulation—applying electrical currents directly to the lower spinal cord—has shown massive promise in allowing paralyzed patients to stand and step. It requires no brain surgery and uses existing pacemaker technology. Yet, it lacks the sci-fi allure of reading minds, so it struggles for the same level of mainstream funding and media spotlight.
The Neural Drift Problem
The media coverage implies that once the computer learns a patient's brain signals, the job is done. The truth is much more chaotic.
The human brain is fluid. It changes how it encodes thoughts from day to day, even hour to hour. A neural pattern recorded on Tuesday morning might look completely different on Thursday afternoon because the patient is tired, caffeinated, or frustrated. This is known as neural drift.
Because of neural drift, the patient cannot simply plug in and go. Every session requires a lengthy recalibration period. The patient must sit still, think about moving their hand while doing nothing, and let the algorithm map their current brain state. If the patient gets frustrated, the emotional noise bleeds into the motor cortex, throwing off the calibration entirely. It is an exhausting mental athletic event, not a seamless integration of thought and action.
The Infection Risk Nobody Talks About
Medical trials are inherently risky, but the public rarely hears about the physical toll of a hardwired brain interface. The wires coming out of the patient's skull represent a permanent break in the skin.
A permanent opening in the scalp is an open invitation for bacteria. Cranial infections are catastrophic; they require removing the implants entirely and treating the patient with heavy doses of antibiotics to prevent meningitis or brain abscesses. While the Feinstein Institutes team followed strict sterile protocols, the long-term management of a transcutaneous port requires obsessive care. It turns the patient's home into a pseudo-hospital room. Wireless data transmission is the obvious goal, but transmitting that volume of neural data wirelessly without overheating the implants—and literally cooking surrounding brain tissue—is a thermal engineering puzzle that remains unsolved.
Managing the Human Toll
The psychological impact on the trial participants is profound. These individuals are heroes who volunteer their bodies for science, but they pay a heavy emotional price.
During lab sessions, the patient experiences a miraculous return of agency. They feel their hand close; they feel the texture of an object. Then, the session ends. The technicians unplug the cables from their head. The system powers down. The patient returns to total paralysis.
This cyclical whiplash—gaining your body back for three hours only to have it stripped away again—takes a psychological toll that few clinical studies quantify. When the trial ends, the implants are eventually removed. The patient is left with memories of movement and a scarred scalp. We must ask whether our current research framework adequately protects these pioneers from the emotional crash that follows the high of technological transcendence.
Moving Past the Hype
The double neural bypass proves that the language of the nervous system can be translated into digital code and back again. It is a monumental proof of concept that deserves its place in the history books of medicine.
But we must stop treating lab successes as immediate medical solutions. To truly democratize this technology, engineering firms must solve the wireless power dilemma, find a way to eliminate neural drift without daily recalibration, and create implants that do not trigger the body's foreign-body response. Until then, this technology remains a brilliant, fragile laboratory experiment—a breathtaking window into the future, but one that is firmly shut for the millions of people who need it today.



